TO THE TREATING DOCTOR
The following appliance explanation is being given at the specific request of the doctor treating the case and is not to be viewed as a treatment plan or diagnosis for the patient. Suggestions are based on records furnished, laboratory work performed and are a recap of discussions with the doctor and do not take into account all diagnostic considerations or any treatment considerations that the doctor may exercise. Any diagnosis or treatment of this patient is solely the responsibility of the doctor treating the patient. These explanations are for the information of the treating dentist only. The explanations provided are not to be considered as any attempt to influence or otherwise interfere with the doctor’s independent professional judgment regarding the diagnosis or treatment of this patient, which is the ultimate responsibility of the treating doctor.
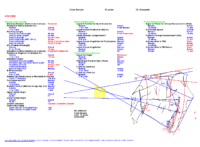
Dr. Sassouni
Regarding: Case Sample (age 12 years)
Concerns for this case according to the cephalometric X-ray and the study models may include:
Maxillary Determinants:
The position of the maxilla is posterior
Adjusted ANS is -10 mm posterior to the anterior arc
The premaxillary length is 10mm, which is short, 3 mm from ideal. (Norm 11-15mm)
Overall, the maxilla is short by -8mm
Mandibular Determinants:
Overall, the mandible is short
Pogonion (front of chin) is -10 mm to the anterior arc
Pogonion (chin button) is short, giving you a small chin button at 5mm. (Norm 6-9mm)
B Point is -2.0mm slightly posterior to A point
Skeletal AP is Class II tendency
Vertical Dimension:
Age Adjusted Skeletal Vertical is 1mm. (Norm -1 to 1 mm)
This patient’s vertical is within the normal range for their age
Growth Direction = Counter Clockwise Growth
Dental Determinants:
The length of the incisor (DAC) is 28 mm, which is short. (Norm 32.5mm)
Upper incisor angulation to the cranial base is protrusive at 117.1°. (Norm 110-113°)
Lower incisor angulation is normal at 92°. (Norm 90-100°)
Summary: B point is 2mm back of the A arc giving you a slight Class II mandible to maxilla, maxilla is 10mm back of the anterior arc giving you a retrognathic maxilla as it relates to Nasion, Class I mandible to maxilla as they relate to one another; premaxilla is reading short at 10mm; B-Perpendicular is small at 5mm which may make the patient look a little Class II; 1mm open vertical to the age adjusted arc, 2mm deep to the cant adjusted arc; patient is a slight counter clockwise grower due to the flat upper Gonial angle of 57°, lower Gonial angle within the norm at 71°; DAC is short at 28mm; normal upper incisors at 112° to the palatal plane and 117° to the optic plane, normal lower incisors at 92°; airway is clear.
Schwarz Korkhaus measurements:
UprRt Central 10mm UprRt Lateral 9mm Upper 4×4 -9mm Lower 4×4 -7mm
UprLt Central 10mm UprLt Lateral 9mm Upper 6×6 -5mm Lower 6×6 -8mm
Study cast: Class II molar right and left; Class II cuspid right and left; dental and skeletal midlines appear to be on.
Possible Appliance Suggestions: Upper memory RPE, lower skeletal, combined with straight wire, possible Rickanator or incisor blocks.
Possible Appliance Therapy: The patient is reading maxilla being back. The profile looks fairly good. Also, the premaxilla is short, but, once again, the premaxilla looks fairly good. The patient has extremely large incisors, especially the laterals that are 9mm. There is a lot of expansion needed. You need about 8mm in the lower, 5mm in the upper molar, and 9mm in the bicuspid area, which you can get the extra expansion with straight wire. Cut the rest off of the bi’s after about 3 months of expansion and allow the straight wire to pull the bi’s out. While expanding, place separators mesial-distal to #29 to allow #29 to come out with bracketing. Go ahead and start right away with bracketing. Wire sequencing will be: .014 thermal, .018 thermal (2 months in each), to an .019 x .025 multi-modulus. Cut the rest off of the bi’s and continue expanding until you get a nice full arch. You may not have to expand the full amount of the Schwarz measurement, which is about 7-8mm on the lower, 5mm in the upper molar, and 9mm in the bi’s. Stay in the .019 x .025 multi-modulus for 4-5 months and move to a mega .019 x .025 CNA rounding out the arch. Once you have retained for about 4 months with the expanders, remove the expanders and evaluate if you need to bring the mandible slightly forward. The mandible might come forward on its own; if not, possibly place incisor blocks and begin verticalization. Figure eight steel ligate lower cuspid to cuspid, place an .016 reverse curve of spee straight leg Niti wire from first molar to first molar for 2-3 months to verticalize, go to an .018 reverse curve straight leg Niti wire for 2-3 months, then go 2-3 months in an .020 x .020 reverse curve. You may get contact of first molars prior to the larger wires. Place separators between the molars and bi’s for 1 week and have the patient remove with tweezers. Repeat this process as often as the patient can tolerate to speed up verticalization. Once you get first molar contact, remove second molar composite, move to an .018 thermal with vertical elastics to the seconds, and finish with an .019 x .025 multi-modulus. Move the upper to an .019 x .025 CNA at any time during the verticalization process. After case is completed, you can reduce the size of the incisor blocks, but leave incisor blocks for at least 6 months to stabilize the verticalization. For overall treatment time for this case is about 2 years. Once the case is completed, retain with Hawley retainers.
All supplies mentioned in treatment recommendations can be supplied by Five Star Orthodontic’s supply department. Please go to www.fivestarortho.com for our online catalog and excellent pricing.
All explanations and observations are given solely at the request of and based solely upon the information provided by the treating doctor. Any diagnosis and treatment should be based on the treating doctor’s independent professional judgment without regard to the foregoing explanation or observations.